Cardio Pump
First Response Australia

The CardioPump permits the rescuer to actively re-expand the chest during the decompression phase of cardiopulmonary resuscitation (CPR). Active compression decompression CPR (ACD CPR) enhances the intrathoracic vacuum (negative pressure) during chest wall recoil, resulting in more blood being returned to the heart (preload). Enhanced preload leads to increased cardiac output on the subsequent chest compression.
The design of the device allows the rescuer to use the same position and compression technique as for standard CPR. The suction cup sticks to the chest and transfers a lifting force to the thorax. Active chest decompression is obtained simply when the operator swings their body weight upwardsafter each compression while holding on to the CardioPump handle. Chest compression is accomplished in the same manner as for standard manual CPR by pushing down on theCardioPump.
When ACD CPR is performed in conjunction with the ResQPOD Impedance Threshold Device (ITD), hemodynamics are further improved.
Technical Specifications
Dimensions
Suction cup: 135 mm OD
Handle: 143 x 108 mm
Weight: 0.58 kg (1.24 lbs)
Gauge
range:
Compression: 0-50 kg (0-110 lbs)
Decompression: 0-15 kg (0-33 lbs)
Accuracy: +/- 10% of reading
Operating temperature range: -20 degrees C to 50 degrees C
Storage temperature range: -40 degrees C to 70 degrees C
Metronome
Function
Signal pitches: 768 and 3070 Hz
Sound level: 65 dB at 0.5 m from the sound source
Signal rate: 80 signals per minute
Battery life: Approx. 250 service hours
Battery shelf life: Approx. 10 years
Materials
Suction cup: Silicone rubber
Handle: Polyamide (nylon), glass fiber reinforced
Metal parts: Stainless steel, brass
The CardioPump does
not contain latex.

Active Compression Decompression (ACD) CPR
ACD CPR
is recommended in the American
Hearth Association Guidelines as an alternative
to conventional standard manual CPR.
In-hospital and out-of-hospital studies* have shown that performing ACD CPR:
- Increases arterial blood pressure
- Increases coronary perfusion pressure
- Lowers intrathoracic pressure during the decompression phase of CPR
- Increases short-term and long-term survival rates

CardioPump Components:
Suction
Cup - provides the suction necessary to actively lift
the chest during decompression. A compression pad located
inside helps cushion the surface between the chest and the
device.
Handle - transfers force from the rescuer to the
victim through the piston
Force Gauge - guides both compression and
decompression forces
Metronome - guides proper compression/
decompression rate and duty cycle
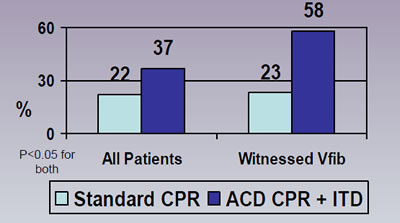
Survival to 24 Hours
- Wolcke et al Circulation 2003
References for
ACD CPR:
1. Shultz JJ, et al. Evaluation of standard and ACD CPR in an
acute human model of ventricular fibrillation. Circulation 1994;
89:684-94.
2. Lurie KG, et al. Evaluation of ACD CPR in victims of
out-of-hospital cardiac arrest. JAMA 1994; 271:1405-11.
3. Plaisance P, et al. A comparison of standard CPR and ACD
resuscitation for out-of-hospital cardiac arrest. NEJM
1999;341:569-75.
4. Plaisance P, et al. Benefit of ACD CPR as a prehospital
advanced life support. A randomized multi-center study.
Circulation 1997;95(4):955-61.
5. Mauer DK, et al. Effect of ACD CPR on survival: a combined
analysis using individual patient data. Resuscitation
1999;41:249-56.
ACD CPR with an impedance threshold device (ITD) (e.g.
ResQPOD):
6. Wolcke BB, et al. Comparison of standard CPR versus the
combination of ACD CPR and an ITD for out-of-hospital cardiac
arrest. Circulation 2003;108(18):2201-5.
7. Plaisance P, et al. Inspiratory impedance during ACD CPR: a
randomized evaluation in patients in cardiac arrest. Circulation
2000;101(9):989-94.
8. Plaisance P, et al. Evaluation of an ITD in patients
receiving ACD CPR for out of hospital cardiac arrest.
Resuscitation 2004;61(3):265-71.
9. Plaisance P, et al. Use of an inspiratory ITD on a facemask
and ET tube to reduce intrathoracic pressures during the
decompression phase of ACD
www.advancedcirculatory.com CPR. Crit Care Med 2005;33(5):990-4.